
Estrogen Is A Longevity Medicine
And There Is Science To Prove It
A position statement from Willbe. on the science we can no longer afford to ignore, the women who deserve better, and why the conversation about HRT needs to change.
Dr. Vanessa Emslie, PhD and Yulia Minchin, B.Sc
THE STATEMENT WILLBE. STANDS BEHIND: Estrogen helps improve Healthspan and should be considered a Longevity Medicine
We say this not as a marketing line, not as a provocation, and not as a fringe position held by hormone advocates on the internet. We say it because the clinical evidence, accumulated across decades, published in the New England Journal of Medicine, JAMA, Nature, and the world’s leading ageing research institutions, say it first.
When estrogen falls during the perimenopausal transition, it does not simply trigger hot flushes and disrupted sleep. It initiates a cascade of measurable, biological changes that impact every major organ system in the body: the heart, the bones, the brain, the muscles, the metabolic pathways, the immune system. Each of those changes are linked to diseases that fall within the category of Chronic Disease, which are widely considered as being preventable.
“When estrogen falls, it does not simply trigger hot flushes. It initiates a cascade of biological changes that medicine has a category for: chronic disease.”
Research has given us clear statistics around chronic disease risks in women:
• The postmenopausal woman is two to six times more likely to develop cardiovascular disease than her premenopausal counterpart. Her LDL rises, her HDL falls, her blood vessels stiffen and her blood pressure climbs, all within the same hormonal window.
• Her bones,maintained for decades by estrogen’s supportive regulation of bone remodelling, begin to dissolve faster than they are rebuilt. One in three women over 50 will develop osteoporosis.
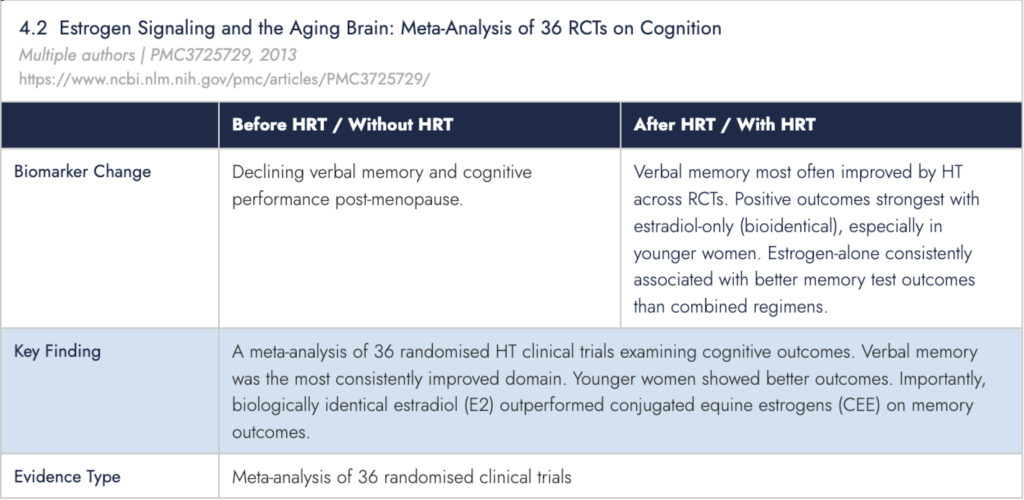
• A woman’s risk of Alzheimer’s disease is nearly double that of a man her age. This disparity is explained by the biological changes of what happens to the female brain when estrogen levels decline post menopause.
These are not quality-of-life inconveniences for women, but are leading causes of death, disability, and diminished healthspan in women over 50 worldwide.
THE NOISE WE NEED TO ADDRESS
We understand why confusion exists. In 2002, the Women’s Health Initiative (WHI) published findings that prompted a generation of women to abandon Hormone Replacement Therapy (HRT) overnight. HRT use fell by more than 50% in the years that followed, and the conversation about women’s hormonal health was set back by at least a decade.
What has become clear in the years since after through re-analysis, longer follow-ups, and a far more nuanced understanding of formulation, route of administration, and timing, is that the original WHI findings were specific to a particular population (women aged 50–79, many of whom were years post-menopause) using a particular formulation (oral conjugated equine estrogens combined with synthetic progestins). The findings should not have been a final verdict on estrogen or HRT usage.
“The WHI was not a verdict on estrogen. It was a finding about a specific formulation, in a specific population, at a specific time. Unfortunately, it has been misread ever since.”
The result is that for years, millions of women worldwide navigated the perimenopausal transition without informed hormonal support because the headline from 2002 echoed louder than the science that followed it. That began to change in October 2025, when the FDA removed the black box warning from estrogen prescription products, formally acknowledging what the clinical evidence had been showing for years.
The response to this shift in FDA labelling has been immediate and immense: by May 2026, estrogen patch usage had increased by approximately 26%, a surge significant enough to trigger a national shortage. Women, it turns out, were never indifferent to their own health. They were simply waiting for medicine to stop scaring them away from it.
WHAT THE EVIDENCE ACTUALLY SHOWS
The evidence that Willbe. forms its belief that Estrogen is a Longevity Medicine, is not anecdotal, speculative, or from the observations of medical practice. It is peer-reviewed, multi-centre, and reproducible.
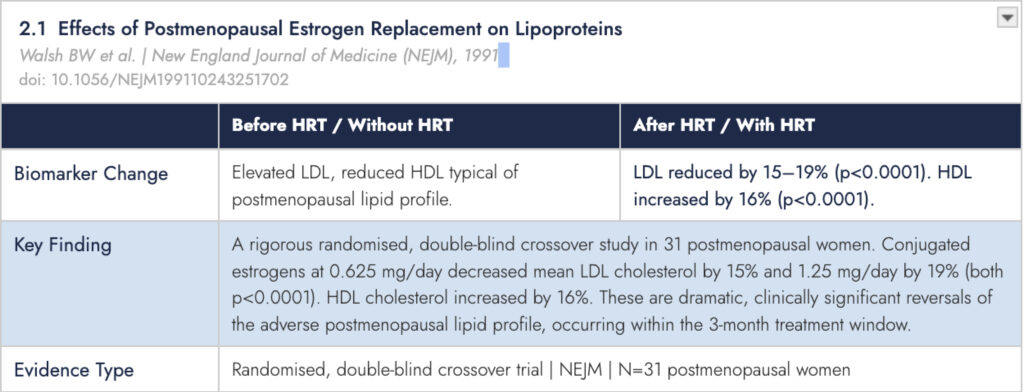
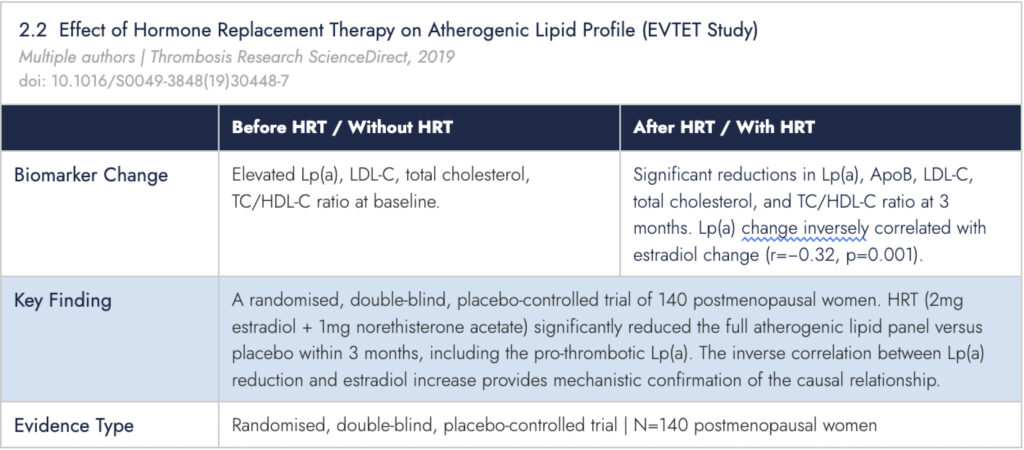
• On cardiovascular health: a landmark randomised, double-blind crossover trial published in the New England Journal of Medicine demonstrated that estrogen replacement reduced LDL cholesterol by 15–19% and raised HDL by 16% in postmenopausal women. A separate RCT found significant reductions in Lp(a) (one of the most potent independent markers of cardiovascular risk) within three months of HRT initiation, with the reduction inversely correlated with rising estradiol levels.
• On bone: the Women’s Health Initiative hormone therapy arm found bone mass density increased by 3.7% in women on HRT versus 0.14% in those on placebo after three years. Hip fracture protection from estrogen-only therapy persisted for 13.2 years post-treatment, a structural legacy effect of estrogen that extends well beyond the period of use, plus improved muscle mass, which supports optimal bone health and mobility..
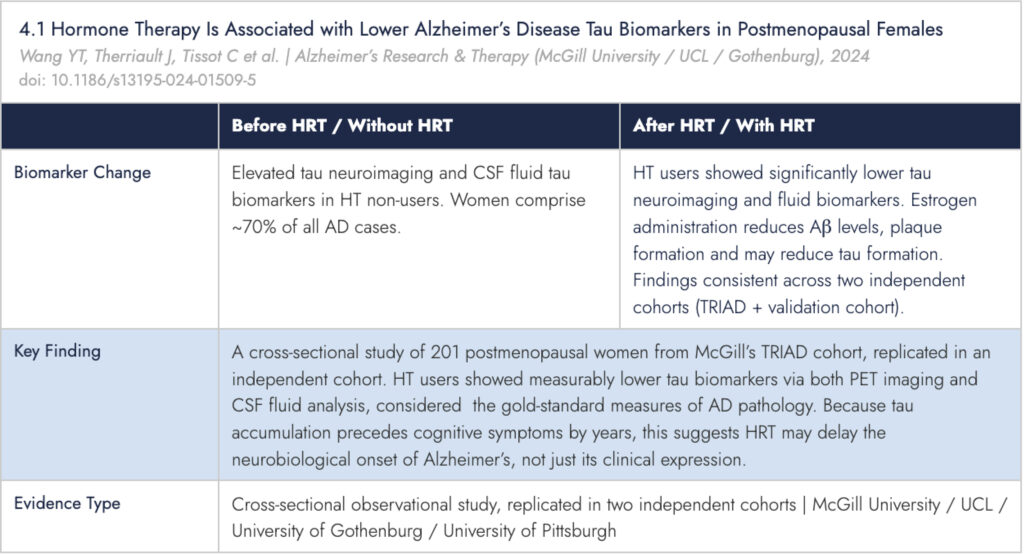
• On the brain: researchers at McGill University, working across two independent cohorts, found that postmenopausal women on hormone therapy had measurably lower levels of tau (considered a pathological biomarker of Alzheimer’s disease) compared to non-users. Tau accumulates in the brain years before any cognitive symptom appears. If estrogen reduces tau burden, it is not merely treating menopause, it is potentially delaying the biological onset of one of the most feared diseases that burden women and their families.
“Postmenopausal women on HRT had measurably lower levels of tau, considered the hallmark biomarker of Alzheimer’s. Estrogen may not just treat menopause. It may delay the biological pathways of dementia.”
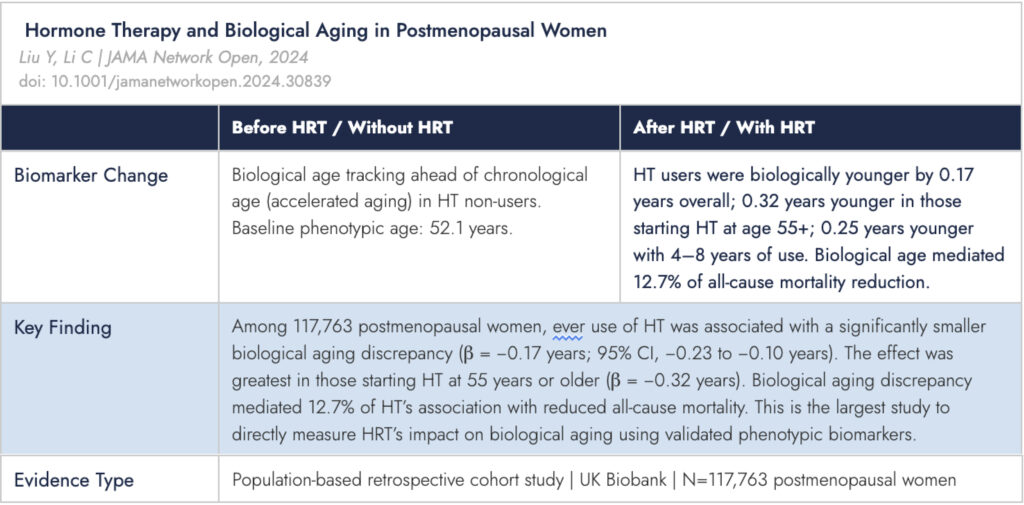
• On biological aging: a 2024 study published in JAMA Network Open, drawing on data from 117,763 postmenopausal women in the UK Biobank, found that women who had used hormone therapy were biologically younger than those who had not. This was measured not by self-report, but by nine validated blood biomarkers that have been linked to mortality risk. The biological aging benefit mediated 12.7% of HRT’s association with reduced all-cause mortality.
“Hormones don’t just treat symptoms — they can protect your bones, brain, and heart, helping women live longer, healthier lives.”
Dr. Kelly Casperson, MD (Innovate & Elevate Podcast, 2026)
These are not small signals. They are a growing body of evidence that, taken together, makes a coherent and compelling case: that estrogen does not merely manage symptoms, iIt maintains systems.
WHAT WE MEAN WHEN WE SAY ‘HEALTHSPAN AND LONGEVITY MEDICINE’
Improving Healthspan through Longevity Medicine is not about living forever. It is about compressing morbidity, spending more of your years living well and active, and fewer of them in decline, placing burden emotionally, financially and socially on yourself, family and the medical community.
By that definition, estrogen is among the most powerful tools available to the perimenopausal woman to improve her healthspan. It protects the cardiovascular system from the lipid and vascular changes that precede heart disease. It maintains skeletal integrity in the decade when bone loss accelerates most sharply. It preserves neurological architecture at the precise window when Alzheimer’s pathology begins to take hold. It supports muscle mass, metabolic flexibility, mood regulation, sleep architecture, and immune function.
The question is not whether estrogen improves healthspan, or is a longevity medicine, it’s rather why it took so long to say so out loud.
“Estrogen is the billion-dollar longevity drug we’ve been seeking for decades — but we already have it, and it costs less than $30 a month.”
Dr. Amy B. Killen, MD (via Alloy Health webinar, 2025)
THE WILLBE. POSITION
Willbe. was founded on a simple premise: that women deserve precision, not guesswork, when it comes to their hormonal health. FemGene® exists because of the way HRT is currently prescribed: one protocol for every woman, regardless of her genetics, her metabolic pathways, her receptor sensitivity, or her symptom profile, which is not good enough.
Willbe. supports the use of bioidentical HRT when it is clinically appropriate, individually tailored, and actively monitored. However, we do not support the blanket avoidance of estrogen driven by a misreading of 20-year-old data; plus we do not believe that the women in our care should be left to navigate one of the most biologically significant transitions of their lives without the information and support they need to make genuinely informed decisions.
“Willbe. does not believe women should navigate one of the most biologically significant transitions of their lives without the information to make genuinely informed decisions.”
We also want to be clear about what Willbe. is not saying. We are not saying that HRT is appropriate for every woman nor are we dismissing clinical nuances around timing, formulation, route of administration, or contraindications. The timing hypothesis, that HRT initiated within five to ten years of menopause onset carries the greatest benefit and the lowest risk, is a key part of the clinical picture.
• Precision matters.
• Monitoring matters.
• Informed consent matters.
But none of these real, important nuances should be used to justify what has become the default: doing little, saying nothing, and leaving women to believe that what is happening to their bodies is simply ageing; when in fact it there are ways to manage a significant biological process with a clear mechanistic explanation and an increasingly robust evidence base for intervention.
THE CONVERSATION THAT NEEDS TO HAPPEN NOW
The perimenopausal transition affects every woman who lives long enough to reach it. Over 47 million women enter it annually. More than 70% of them will experience musculoskeletal symptoms. A third will develop osteoporosis. Two thirds will develop cardiovascular disease. And women will develop Alzheimer’s disease at nearly double the rate of men, typically after menopause.
“Estrogen is not just about fertility — it’s a key player in longevity, brain function, and optimal cardiovascular health.”
Dr. Jolene Brighten, NMD (DrBrighten.com, 2024)
Willbe. has a tool that addresses the biological root of all of this, plus we have the evidence to support it. Through a clinical framework developed through FemGene®, we can implement HRT with the precision and monitoring women deserve.
The statement ‘estrogen helps improve healthspan and is a longevity medicine’ is a clinical position grounded in peer-reviewed evidence from the world’s leading research institutions. And it is one that Willbe. is here to discuss, in the clinic, in the press, and with women who deserve more from their current hormonal healthcare journey.
We invite clinicians, researchers, journalists, and policymakers to engage and discuss the evidence.
FEMGENE® | CLINICAL DATA STATEMENT — ADDENDUM
HRT & Estrogen: Evidence for Reversal of Age-Related Biomarkers
The studies below provide direct clinical and biomarker evidence that estrogen, when introduced responsibly and critically via HRT, can show measurable reversing or attenuating of age-related biological changes driven by the menopause transition. These findings support the position that estrogen is not merely symptomatic relief, but a tool capable of modifying the trajectory of biological ageing and improving Healthspan.
IMPORTANT CLINICAL NUANCE: THE TIMING HYPOTHESIS
Several of these studies confirm the ‘timing hypothesis’: that the greatest biomarker reversal, and the lowest potential risk, occurs when HRT is initiated within 5–10 years of menopause onset, or before age 60. This is clinically critical context for any reader, public or press statement. Willbe. supports the evidence-based, personalised and monitored use of HRT, not a universal one-size-fits-all prescription.
1. BIOLOGICAL AGEING IS ASSOCIATED WITH A MEASURABLY YOUNGER BIOLOGICAL AGE
The Landmark Finding
The most direct evidence for estrogen as a longevity medicine comes from a 2024 JAMA Network Open study using UK Biobank data from 117,763 postmenopausal women. Biological age was calculated from nine mortality-associated biomarkers and compared to chronological age.
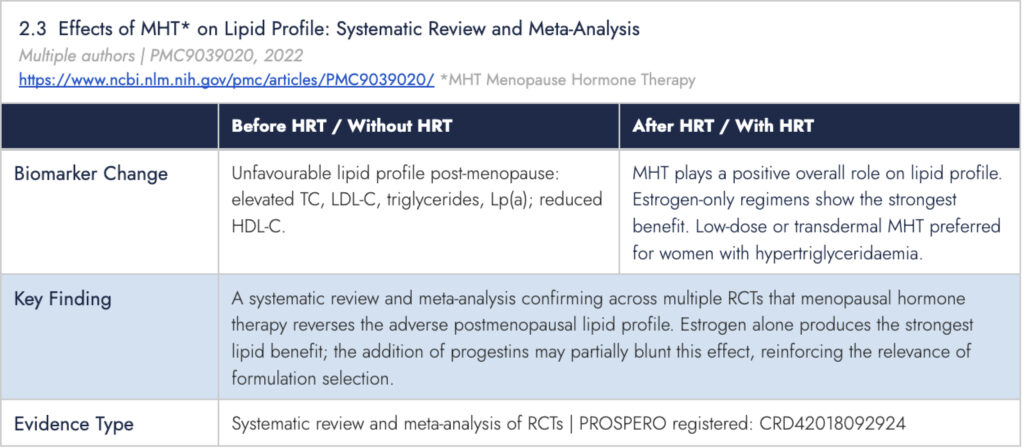
2. CARDIOVASCULAR BIOMARKERS: CHOLESTEROL, LDL, HDL & LP(A) REVERSAL
The Mechanism
The most direct evidence for estrogen as a longevity medicine comes from a 2024 JAMA Network Open study using UK Biobank data from 117,763 postmenopausal women. Biological age was calculated from nine mortality-associated biomarkers and compared to chronological age.
4. BRAIN & ALZHEIMER’S BIOMARKERS: TAU & AMYLOID REDUCTION
The Mechanism
Tau tangles and amyloid-β plaques are the hallmark pathological biomarkers of Alzheimer’s disease — and they accumulate years before symptoms emerge. The studies below show that HT use in postmenopausal women is associated with meaningfully lower levels of these brain biomarkers, consistent with estrogen’s neuroprotective mechanisms.
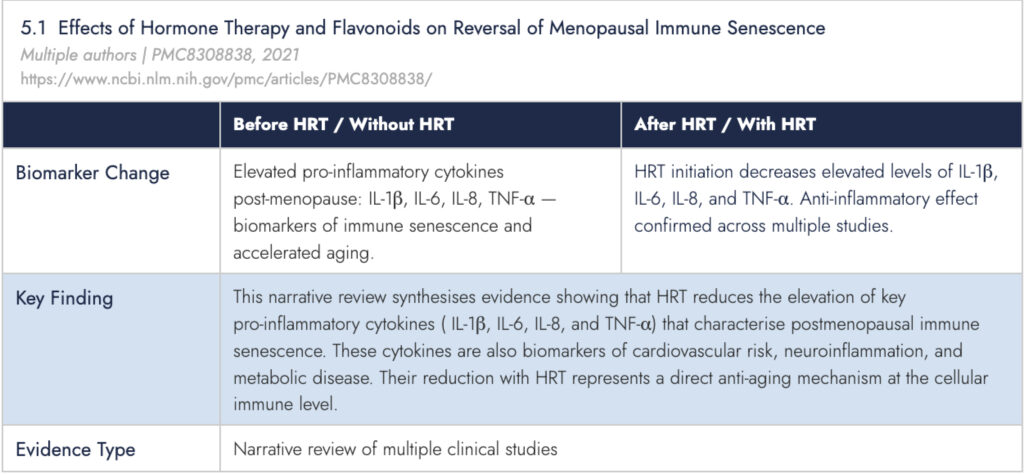
5. INFLAMMATORY BIOMARKERS: REVERSAL OF IMMUNE SENESCENCE
The Mechanism
Chronic low-grade inflammation or ‘inflammaging’, is considered a core driver of multiple age-related chronic diseases. Menopause accelerates this inflammatory state via the loss of estrogen’s anti-inflammatory regulation. HRT has been shown in research to reduce key pro-inflammatory cytokines that track with biological aging and disease risk.
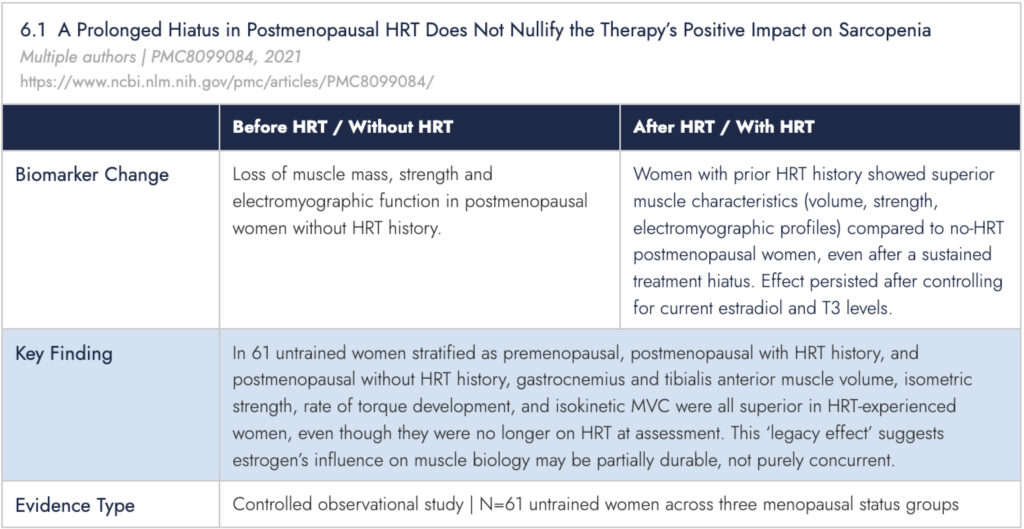
6. MUSCLE MASS & PHYSICAL FUNCTION: HRT LEGACY EFFECT
The Mechanism
Estrogen regulates satellite cell (muscle stem cell) proliferation, mitochondrial function in skeletal muscle, and anabolic signalling. Its loss accelerates sarcopenia. HRT use has been shown to preserve muscle characteristics — with evidence suggesting benefits persist even after discontinuation.
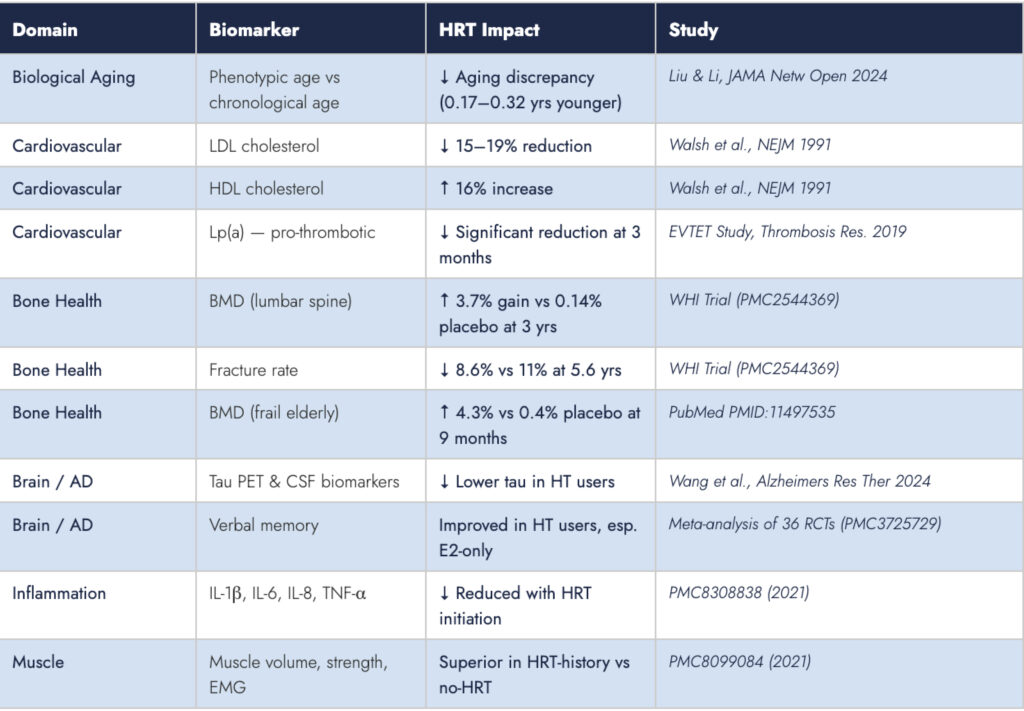
SUMMARY: BIOMARKER REVERSAL BY DOMAIN
ADDITIONAL CITATIONS
1. Whitepaper: Hormogenomics ™ & Hormogenetics ™ 2025, available from Willbe.
2. Global Lifespan Gaps. doi:10.1001/jamanetworkopen.2024.50241
3. Society for Women’s Health Research, 2019
IMPORTANT CONSIDERATION
This document provides a curated evidence base for clinical and press reference. It does not constitute prescribing advice. All HRT decisions must remain under clinician authority and prescribed based on the clinical case and preconditions. The studies referenced include observational, cohort, and randomised controlled designs; the strength of conclusions should be interpreted in line with the evidence type noted for each citation.
– STATEMENT END –